


Some things that I do not know

There are actually is quite a wide range of topics I do not know a whole lot about, but to try to keep this in substack length limit range, we’ll try to limit the scope a bit. I’m not entirely sure what I’m trying to do with this post necessarily, but from my side putting these posts together is to try to do some level of the self review you have to do when you sit down and write something. It seemed like a useful exercise to try to lay some of this out, in the interest of working on moving the dial more towards known. There was a time when I could quickly dial up a description from the CDC or even news outlets with some assurance the answers were accurate. We don’t seem to be in that place anymore, so we now have to go spend hours better spent elsewhere trying to make sense of things. So OK — here goes.
Are the vaccines safe (or safe enough) or not?
I lean more towards “not” than “safe”. My “lick finger and stick in the air” sense of this at the moment is perhaps they don’t look quite as dire as in the early spring, when adverse reports were streaming in during the peak of the US vaccination surge. “Useful” or “A good idea to deploy widely” are different questions that maybe I’m starting to have a handle on. “Safe” though… one need only look at the openvaers1 site to see the alarming numbers of reports and deaths coincident with vaccination to trigger a “WTF?”. At this writing they have 13,911 reported deaths out of 22,792 total. The COVID death report number is an alarming 61% of the total for all vaccines and all the 30 or so years VAERS has existed. I’ve at least spent some time fiddling with the VAERS data, trying to understand what it says. I find I can mostly reproduce the openvaers numbers if I include both “domestic” and “non-domestic” VAERS reports. Let me explain a bit.
VAERS2 is a system the US government established to enable reporting of adverse effects from vaccines. The system provides data going all the way back to 1990 or so, when that effort started. The data are public, are in annual csv files — essentially spreadsheets, for 3 sorts of data “VAX”, “DATA”, “SYMPTOMS”. Beyond the yearly sets of files, there is an additional set labeled “nondomestic”. These it appears are reports from outside the US that US drug manufacturers receive and must report. I tend not to use them since I’m interested in what’s up in the US, but do pull them in occasionally to “bug check” against the openvaers site numbers.
The entries in each year and the non-domestic sets of csv files are linked to individuals or cases by “VAERS ID”s. There actually is a wealth of information the files, but a lot of it is free form text that doctors (and it looks like some patients) have entered in by hand. Free form human readable text is a hard thing to try to analytically deal with. There are also dates, names of vaccines, simpler things to key off of to make some straightforward counts and plots.
The data includes reports for all vaccines, including flu and the ones we get as kids, all conveniently labeled. There’s an avalanche of entries for COVID in particular though, definitely much more than for flu vaccines. I can cook up some simple code to read all of these files, tie entries together by VAERS ID, and do some rudimentary analysis on them. If I do not include the “non-domestic” data, I think constraining reports to USA, I only have half the amount of deaths listed on the openvaers page. I interpret this to mean in the USA there’s about 6k fatality reports with some association to a COVID vaccine. Reading the free form text of several of them, a lot of them “by eye” really look to be related to the covid vaccines. Often they are immediate reactions from the shot before the individual leaves the vaccination site.
There are flags in the CSV’s for whether an entry is a death record, and several dates relative to the time of vaccination. First thing I did here is plot the date of deaths in the database and eyeballed that vs the US vaccination time distribution in ourworldindata.org3.


Above are two plots, the top in blue is from the VAERS domestic data, and bottom in green is plot of vaccination dates for US cases. The shapes are subjectively similar, so that tells me there does appear to be a relation between the two. The VAERS data is not just random entries from 15 year olds playing around. But in some sense that it be connected to vaccinations would have to be by definition. An entry there is certainly only going to happen in association with a vaccine having been applied. (Watching for “patient bit tongue and bled to death upon trying to figure out how to pronounce Comirnaty” though) On top of that, more than likely a doctor is only going to think to enter when it’s pretty clear it’s related. Like for example in office, right after the shot. 2 months later? Who knows. And indeed if you look at the time difference between the entry and the shot time they’re primarily within a few days of each other.
What are the long term effects of the vaccines we have to worry about?
An important question here too if you look at the age distribution of these people, you see the most common age for fatalities about 80 years old. Which is actually not unlike the fatalities from the disease itself. Or well, life in general. You spend your whole life working to eventually become one of these 80+ year olds, only to find the survival rate once you get there is terrible. Part of the uncertainty of this then is, are these people who were about to die anyway? Just on the precipice, and happened to pass away a day or two after they got the shots? Is this distribution just a tautology? Why then is it so much — I believe some large factor (need to check this) more than all flu shots combined? The “just happened to die after a shot” should equally apply to all other vaccinations — why so much here? Ah and:
To what extent are the COVID disease fatalities themselves a direct mapping of the “about to die anyway” population?
Possibly a next step here would be to try to estimate how many entries you would expect to get under the “people that just happened to die after the shot” scenario. There are some web “Insurance-y” tools around that might give some numbers to base this off of. pip install whenamIgoingtodieanyway comes up empty though.
So on one hand we have an unprecedented quantity of reports in this database, but then deaths seemed to track the vaccination dates, and since the initial flurry of vaccinations have waned since the summer, have also more or less slowed to a trickle. Though that with active censorship of these sorts of reports at a level evoking Fahrenheit 451 or 1984….
What exactly BTW, is the definition of “misinformation”?
And why hasn’t this newfound enthusiasm for withholding questionable ideas from people to protect them been applied to save people from things like Flat Earth Theory4. Sorry — scope creep. On the surface, if one believes the documented scale, in terms of deaths, vaccinations (according to VAERS) are not even in the top 10 causes in the US. Much more than lightning strikes5, but two orders of magnitude below the largest source of death in the US, heart disease6. (Or COVID itself). Still don’t understand this, have also not had time to really dig into the hundreds of thousands of nonfatal, yet severe reports in this data.
Could severe side effects be dependent on vaccine delivery? I.e. injected into bloodstream?
I do wonder to what extent severe effects that are happening are related to the vaccinator (word I think I just made up for the person giving the shot) happening to inject the vaccine into the bloodstream rather than into muscle tissue. I wonder this, having in the past had to figure out how to inject medicine into a squeamish family member each day for some number of weeks. A lot of strange things can happen when medicine is injected into a person by less than the best trained hands (Though I’m sure the swarm of vaccinators who sprang up in the parking lots of America were all incredibly well trained). I know I definitely hit veins, heard complaints they could suddenly taste what I had injected (this was an effect our nurse confirmed was actually something that they know about but don’t have an explanation for), despite my best attempts not to screw that up. What happens if a covid vaccine accidentally gets injected into a vein through no real fault of the vaccinator? Not disputing that hanging an arm out a car window is the best way to get a shot delivered. Does subcutaneous injection (which BTW they do for some flu vaccines) make this less likely than the current intramuscular injection?
Do masks really work?
I will be honest here — we’re very pro mask in this house. A large part of this is memories of SARS 1, but also the use of masks (in part due to SARS 1 but also past flu epi/pandemics) is accepted practice in Asia. In Japan you wear a mask out of politeness toward others when you have a cold, or even if you are sneezing from seasonal allergies. They work. We know this. Doctors know this. Masks as a means to stop the spread of pathogens has been known to medicine for centuries. That there is debate over this is… weird. I wonder how much of this could have come from China buying out the US, if not world mask supply in the beginning of 2020. Personally we were looking to stock up at that time, and could not find them in any stores. ANY. I wouldn’t be surprised at that being at the root of some flip-flopping on the utility of masks early on. Keep the store riots under control (as ironic as that sounds) by playing down the ineffective masks that somehow have all disappeared?
What really happened to mask supplies in the US in the winter of 2020?
That masks can inhibit or prevent an infected person from spreading disease to others is well known, the question is are they of use to protect someone from receiving the disease. We believe so, and have engineered our own masks to fit our faces without gaps, have pockets to slip in N95 filters, etc. We wear them when we depart our property, drop them in a box in the laundry when we come home and wash them each day. It’s honestly a pain in the ass, but the advantage to this is when you get home you can remove them, unlike a vaccine. AND they should work equally well on Flu and colds. Remember those? So far none of us in this house have had so much as a cold for the last year and a half (knock on wood). Keeping hands washed and masking up has been a good formula for avoiding this as well. I am still tying together maybe a future post on this, so thats why I leave the mask question as a question…
What is going on in Japan?
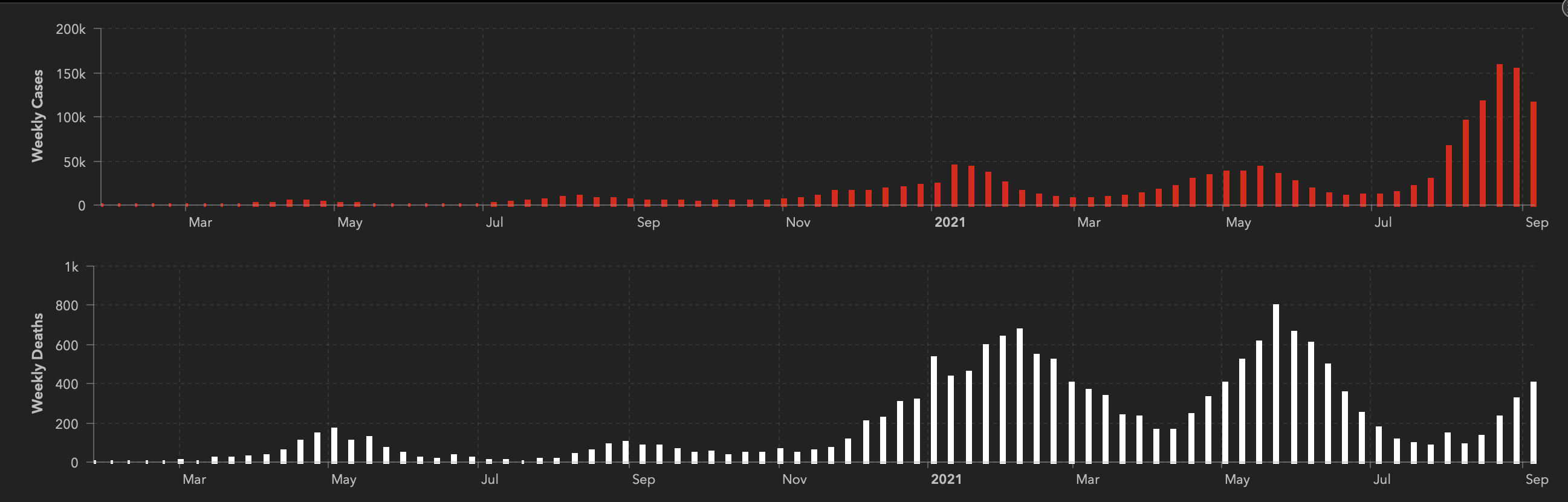
Japan is hopefully coming out of its first real outbreak of the pandemic7. In general despite its proximity to the COVID Mother Country, it has kept this thing at bay without really locking down. Below is the plot of cases and deaths from COVID for the entire pandemic period from JHU, and you can see what is happening currently is the worst so far for them (well in terms of cases. Fatalities, fingers crossed, we hope stays low). For scale though compare to the US, where we’re seeing 10x the number of cases, and 20x the number of deaths (so far). That the cases in Japan have jumped up, but that deaths are possibly lower than even the previous smaller case bumps is very puzzling (but maybe in a good way).
For the low level of outbreaks though, I think I have some idea — in Japan they accept the utility of masks. They wear them, have used them as needed during cold and flu season even pre covid. They also understand the importance of simple things like hand washing. You will almost always get a nice warm cloth to wash your hands before your meal at a restaurant in Japan. They remove their shoes before tracking whatever they walked through in that public restroom, or garage, or whatever, into their homes, onto the floor they sit and their kids crawl on. They bow, keep personal distance when greeting rather than contact hands or rub faces. It seems less mysterious that the Japanese are less affected by something like this, but it is also a bit of a head scratcher why this latest outbreak is behaving as it is. It is at least very good to see a trend toward lower fatality rates! The downward trend in death rates could point to Japan getting a better handle on therapeutic treatments?
Mu and Lambda variants?
I’m pretty sure we’re seeing Delta8 is breaking through vaccinations, cutting their effectiveness down 20-25% points. Two variants popping up in the news are Mu9 (B.1.621) and Lambda10 (C.37). Here’s another place WHO really dropped the ball by the way, using the limited set of Greek characters — Chinese characters seems much more appropriate and better suited to the task. Plus possibly affords the opportunity of naming the worst variants after actual cusswords. Anyway, both Mu and Lambda apparently have mutations that could make them break past immunity worse that Delta. But at least according to CDC numbers, these are still quite low in the US11, so if they do have that advantage, Delta’s virulence might be beating them anyway. Delta is just everywhere.
The predictions that these other variants become dangerous looks to be based on an understanding of the function of what different pieces of the COVID genome control (I would hope not complete guesses? No idea. Similar understanding governed the spike protein tweaks added into the vaccines?) I would think if they did have a greater edge on the vaccinated population, in the US where the majority is now vaccinated, there’s a wide open field that these variants now have some preferential access to. We should be seeing them take over, but Delta still wins so far.
To what extent is vaccine breakthrough due to immunity decay and what is due to a better virus “toolset”?
If the genetic arguments for Mu and Lambda potentially having a better toolset (which might be completely wrong?) are correct, you should see them working into the active variant mix, particularly among vaccinated that other variants have more trouble with. Whether any particular variant takes over ought to be due to it having some way to beat the others. If you observe these other variants becoming dominant within the vaccinated population in particular, that I would think would be a pretty solid indication they break down the vaccine immunity. Would we have any idea, given that the CDC apparently handicapped tracking of breakthrough cases during the summer (if not still currently)? I also hit some of this is here
Or are the breakthrough infections happening just due to the immunity from vaccine “wearing out”. Due to the body I suppose forgetting the past interaction and becoming less able to defend against what it was supposed to be set up to defend against. Cases correlated with vaccination status and dates would tell us this right away I should think. I haven’t found any of that publicly in the US though. It would take maybe minutes to cook up a breakthrough vs time since vaccination plot if the data was available.
The question here is important though, because it speaks to whether a “just shoot up with another of them” booster strategy makes sense to remind people’s bodies what they need to fight against, or if the genetics of the thing has changed sufficiently that we really need new vaccines or (my suspicion) need to re-think the strategy altogether. Or think in the first place perhaps.
OK — I think its time to close this out — there are a lot of known unknowns here (I almost got out of it without the Rumsfeld quote — that was close). Like I said at the start, there are actually several more things than these I do not know. The kinds of questions here used to be ones that I could go and web surf out some answers over morning tea. That may have been a fog we always just were able to live under before and didn’t know it, but there’s too many cases lately where baldface inaccuracies12 are lobbed out there as fact and defended by hisses and finger points. I will say here too in my case I am not a medical doctor, virologist, play them on TV or stayed in ANY hotel last night, so statements I make here should not be believed. I don’t particularly believe myself, hence the title of this post. I’m lobbing this out there in part to impose the self discipline of trying to play the role of an outside reader while working through these questions. If anyone stumbles on these, ripping them apart (beyond the usual “you’re a poophead” arguments) is fully welcome. I’m I guess going back to scratching my head over some of this, as my and my family’s welfare is clearly not to be blindly placed in other’s hands.
https://www.openvaers.com/
https://vaers.hhs.gov/
Mathieu, E., Ritchie, H., Ortiz-Ospina, E. et al. A global database of COVID-19 vaccinations. Nat Hum Behav (2021)
https://www.npr.org/2020/02/23/808645524/daredevil-mad-mike-hughes-killed-in-crash-of-homemade-rocket
https://www.iii.org/fact-statistic/facts-statistics-lightning
https://www.cdc.gov/nchs/fastats/leading-causes-of-death.htm
https://coronavirus.jhu.edu/map.html
https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/
https://www.medrxiv.org/content/10.1101/2021.05.08.21256619v2
https://www.medrxiv.org/content/10.1101/2021.06.26.21259487v1
https://covid.cdc.gov/covid-data-tracker/#variant-proportions
https://www.whitehouse.gov/