

Prepping for the school checkup
Prepping for the school checkup
Not intending to make anything easy anymore.

Later this week we’ll be bringing the middle boy to the pediatricians office for a health checkup in preparation of his entering middle school. Given we’ve seen what we’ve seen1, we need to do a bit of homework on the shots that will be aimed at us in this visit. We have the following to look forward to according to the schedule:
Tdap
Meningitis (Menactra)
HPV (Gardasil)
I had called ahead to find out what he would be due for, telling them I would need to review anything ahead of time. I will say though at this stage we really have no intention of having anything injected into anybody until some trust is rebuilt. I’m putting what I find out here for others to look at and call me out on, of course with the caveat that I’m not a medical Dr dispensing medical advice. Neither would I be serving that role were I to suggest it unwise to biff yourself in the forehead with an axe handle, but thats a different post.
That said, all 3 boys have had all the requisite shots up to this point. MMR, DTaP, Varicella, Hep A&B… and we may or may not have had any problems with any of these2. In looking at the above list, Tdap looked the most sensible to go with, given they’ve all had their full DTaP sequences in the past (and the oldest had TDaP). Past tolerance is a good empirical sign.
HPV, or Human Papillomavirus Vaccine was listed as optional. One of the selling points for this shot appears to be to prevent cervical cancer. I am not a biologist, but I am fairly confident none of my boys own a cervix, either with stick or automatic transmission. Good. Easy one off the table. We also did not do this one for the oldest pre-covid on those grounds.
Meningitis is an interesting one. I never had this myself (the vaccination or the disease), but do remember an incident at University of a dorm resident passing away suddenly of the disease. I looked up some case by age statistics and found this from our dear friends at the CDC3:
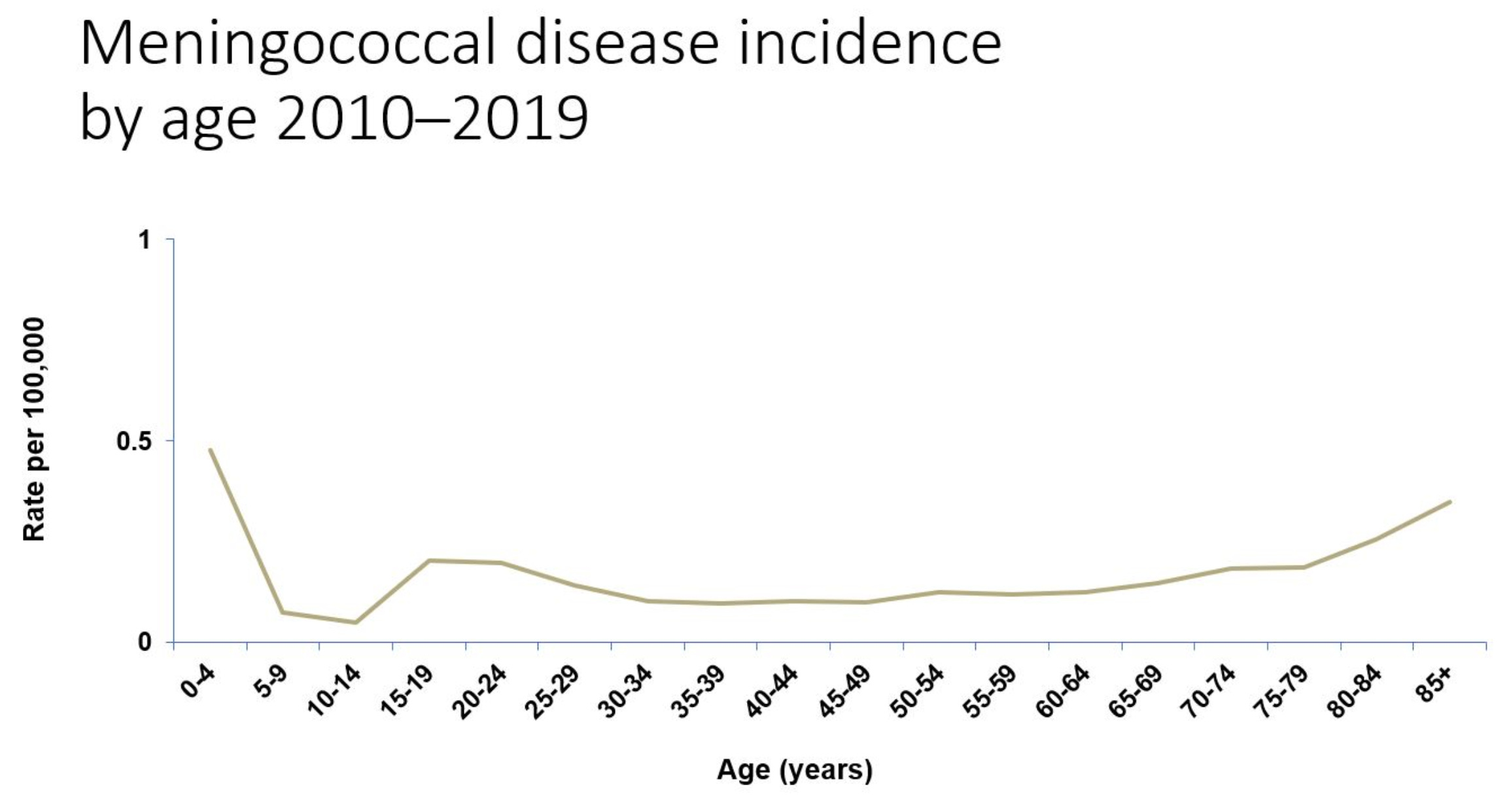
This plot is meningitis case rates by age in the US. Note it bottoms out in the 10-14 age range, right where our soon to be middle schooler sits. So risk of disease for his age group appears low. Note the bump among the college aged, consistent with my anecdotal experience of the dorm resident lost to the disease. As we get closer to that we’ll re-evaluate this risk, but at the moment it looks there is less urgency, according to the CDC.
Let’s roll back to TDaP and look at where we sit with cases in the US for each of the targeted diseases: Tetanus, Diphtheria, and Pertussis. Tetanus is rare, with an average 30 cases in the US per year according to CDC4. They’re quick to point out most of those are among people not up to date with their shots — including adults with their 10 year boosters. I would say I am among this group, it being probably… 20 years since I did this.
Diphtheria is even more rare in the US, with less than one case per year5. Pertussis, or Whooping Cough, though looks to be a different beast — with a few tens of thousands of cases. So OK, that appears at least to be a thing. Here is a plot of incidence per 100k by age group over time from the CDC6.
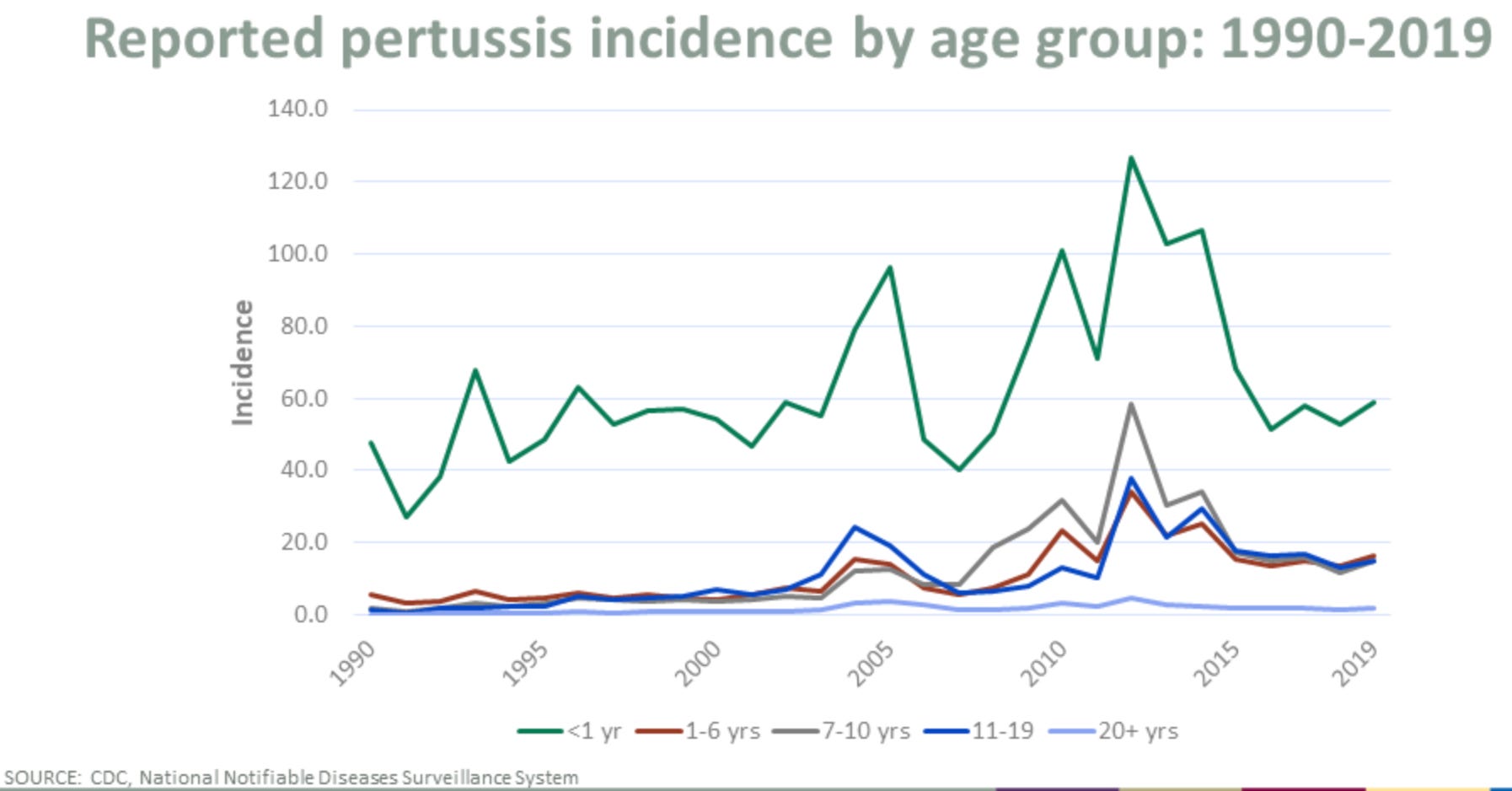
Clearly the majority of cases are in infants, and presumably this is why we’re quick to hit them with several DTaP shots the first couple years. Interestingly the rates in this are not decreasing as years progress. If anything, perhaps the opposite. That will be something to look into, but I also wanted to understand a bit what the disease is. Whooping Cough is a bacterial disease7, which also appears to be treatable with fairly common antibiotics. Lets look a bit how dangerous this is in the United States. The CDC produces annual reports on this, so we’ll take a look at 20198:
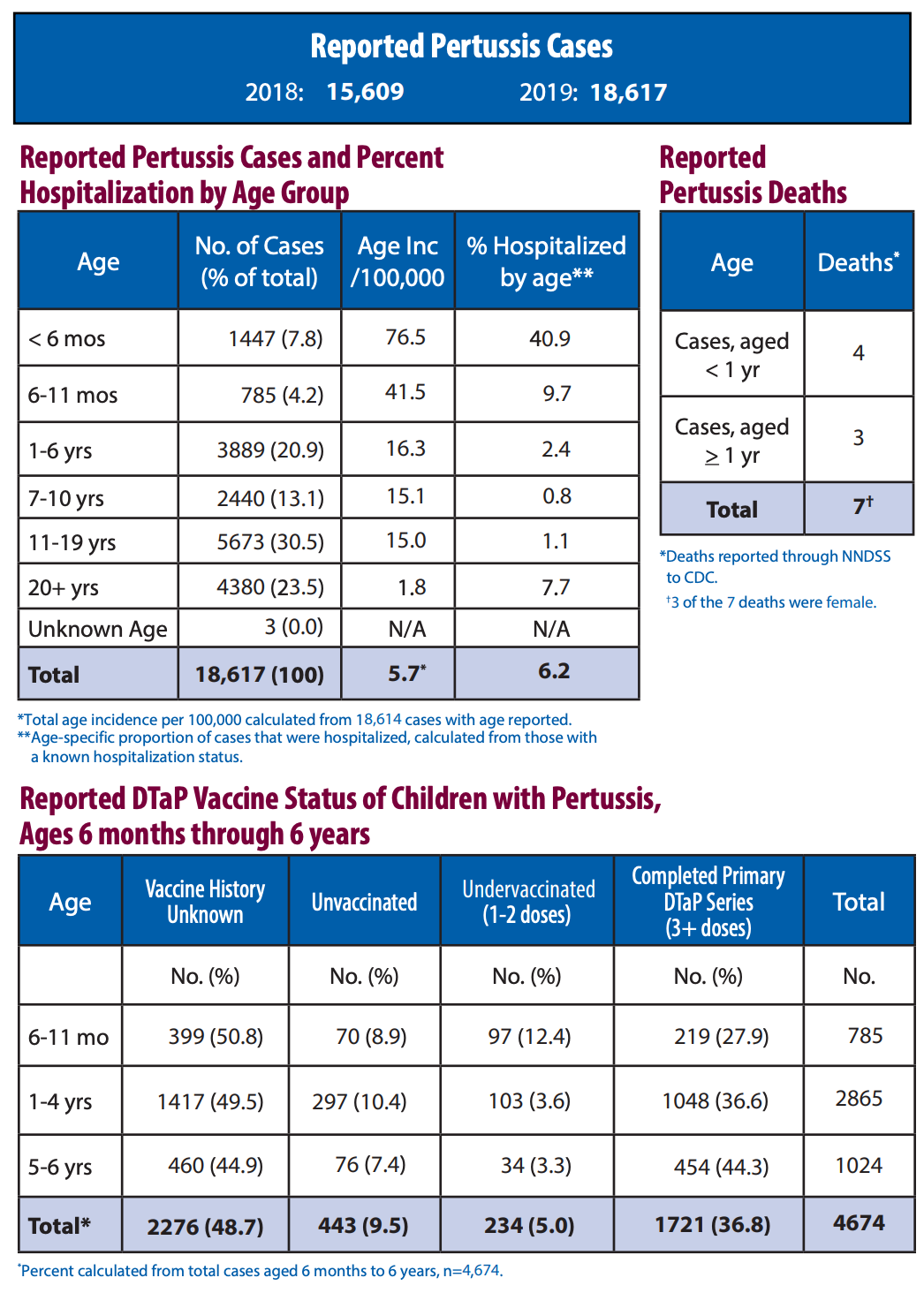
Two things I see right away here:
Out of the ~16k cases among >1 year olds, there were 3 deaths.
Among children through 6 years old with known DTaP vaccine status, the majority of cases appears to be among fully vaccinated children. But we need to be careful here of course — it is likely the vast majority of children are anyway vaccinated. We can loop back here at some point and see if we can work out some efficacy numbers. Particularly digging into other years.
Alright. So this is a thing to be aware of, but seems also not a terrible concern for our age group by these US numbers. I should note were we to be planning to leave the US, where these diseases are not as rare, the risk assessment would likely be quite different. I should also say from the vaccinated numbers above, I do wonder if there is something more to look at here in light of lack of efficacy from other intramuscularly delivered injections for respiratory diseases like flu and covid. Wild-ass armchair guesswork by a fully credentialed wild-ass guesser.
We need to then look at whether the cure is better or worse than the disease. We need to look at VAERS9. The latest data we have includes reports through July 22. For these shots, reports date back a couple decades. Lets look at the counts due to the vaccines we’re being targeted with over time:
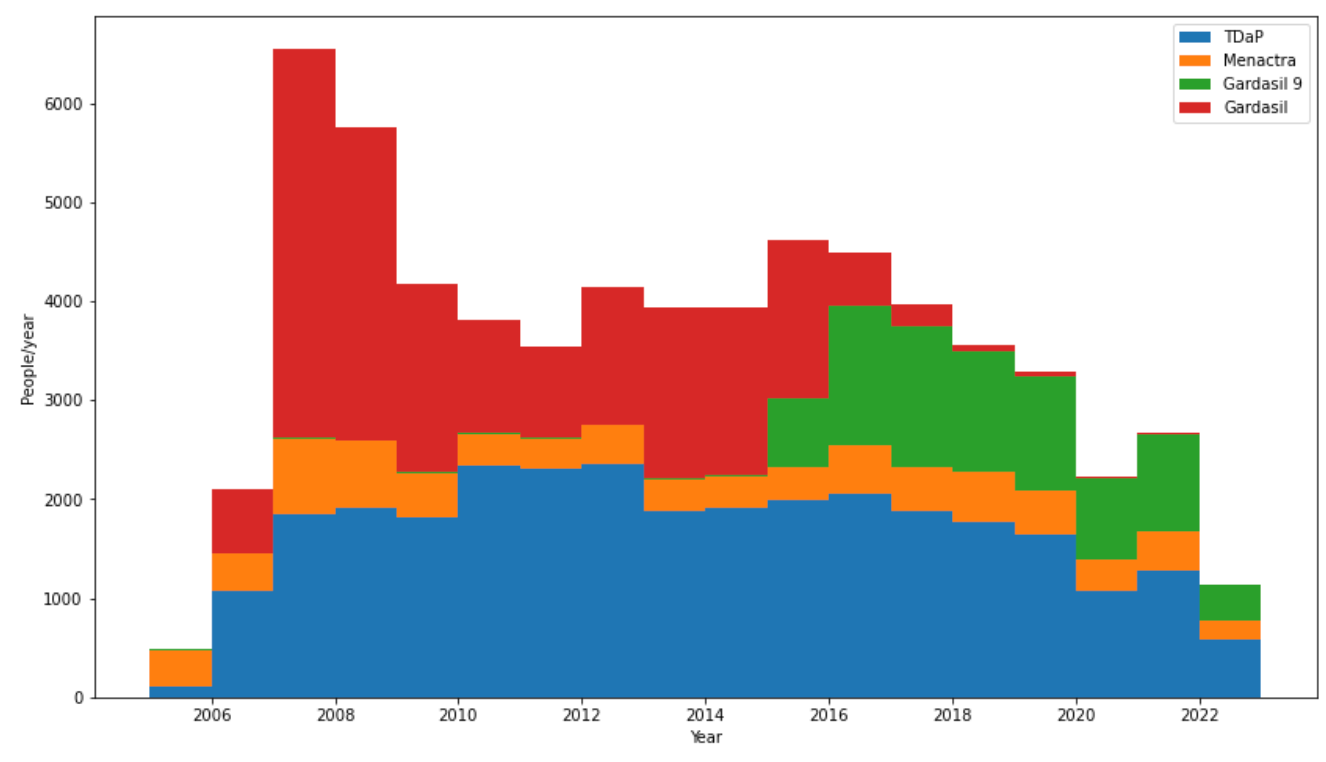
Alright — there are 4 vaccines in this plot, two versions of Gardasil, for HPV, in red and green. We’ve already taken that shot off the table here, but thought it interesting that around 2016 we appear to have changed over from one type to another. When we look at fatalities we’ll perhaps see why. The other two in here are ‘Menactra’, for meningitis in orange, and TDaP in blue. Between the two of those, we’re looking at hundreds of VAERS reports each year.
An aside here thats worth mentioning — note the near constant level of these reports over time, particularly with orange and blue. Then note the drop from 2020 onwards. Keep this in mind if anyone attributes covid entries to a hypothesized increase of VAERS reporting generally in recent years. If anything reporting decreased with the covid lockdowns. There is another interesting observation along these lines: During COVID Lockdown, Vaccine Rates Dropped — So Did the Number of SIDS Deaths. But we digress…
The plot above is just raw entry counts by vaccine type for each year. There is no differentiation in that by year, by age, or by type or severity of adverse event. There also is no normalization by number of shots delivered. The relative magnitudes of each of these could well just be reflective of the frequency of application. An easy indication of severity here at least, that we can try right away, is calling out the entries where ‘DIED’ == ‘Y’. Lets do that:

These are all small numbers. I would say this gives an idea of at least a historical precedent for what has been referred to as ‘safe’10. Look also at the red versus green here — this likely explains the transition from one type of HPV vaccine (HPV4) to another (HPV9) around 2016. Here I would say is a example of a “stopping condition” where one type of vaccine (red) is pulled out of circulation due to an unacceptable rate of severe side effects, in this case apparently unacceptable fatality rates. Note here though fatalities of HPV vaccines appear to improve, but overall reports from the plot further above do not seem to by much. I have not yet dug into what those are or what ages are represented.
VAERS reported fatalities for TDaP and Menactra are small. A handful per year. But then at least in the 2019 Pertussis report we were looking at, 3 deaths for everyone over 1 year old. It would be interesting to see how many >11 year olds are lost to this disease. I would expect that to be a small number. Meningitis fatalities from disease are more significant, with 35 reported deaths in 2019 over all age groups (though 0 in 11-15 year olds)11.
So OK, although there is more I will want to chase here, I think I have enough background to go into the Dr’s office for some discussion this week. It is I suppose encouraging the reported fatalities for these in VAERS are quite low12, but there are a large number of nonfatal reports that I’ll need to understand and dig through yet.
One thing I wanted to do before closing off this particular post though is remake the above plots, adding in the covid shots for perspective — first fatalities:
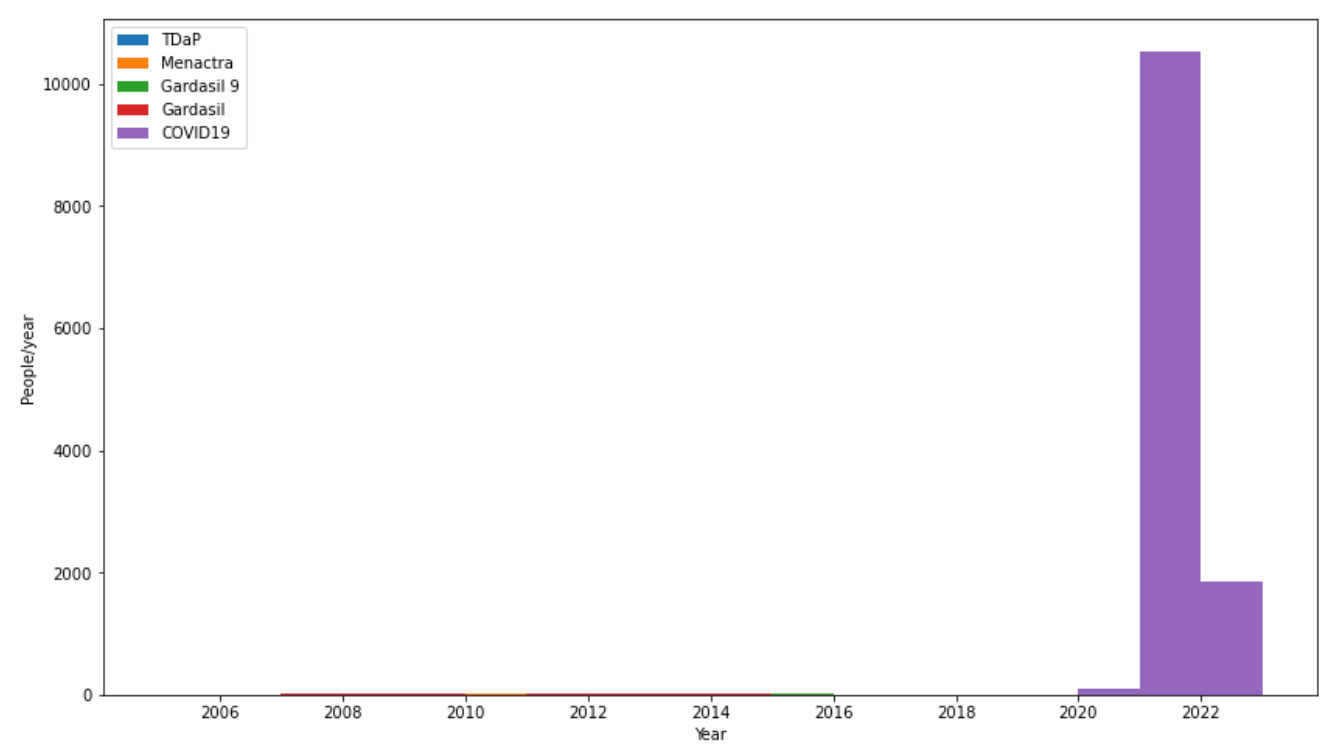
All I’ve done here is add in the covid shot reports, and it completely buries what we’ve talked about above. Including the now invisible Gardasil that was stopped and apparently replaced with a more benign version. For completeness all reports (fatal and nonfatal) for all 5:
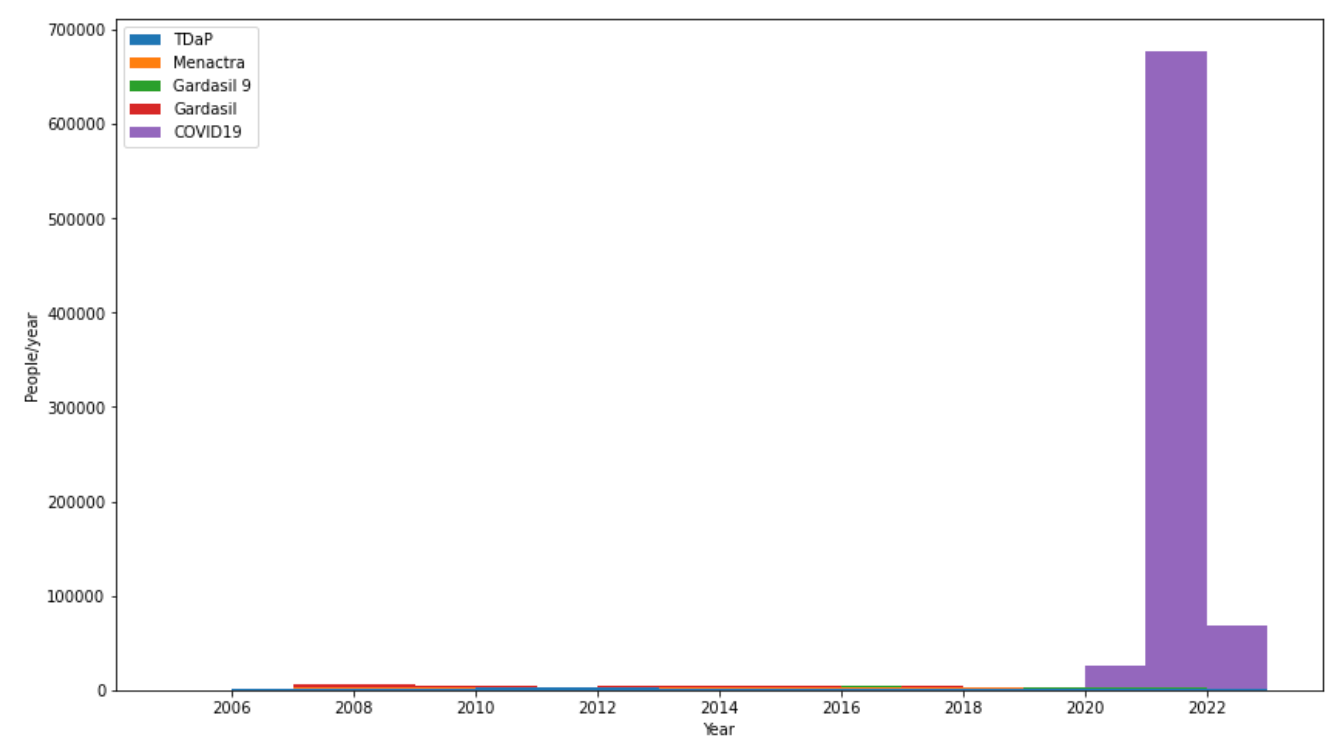
You can perhaps start to see the standard vaccines reappear in this plot, but still very much dominated by covid giving us the middle finger here. Yes, we do still need to look at why covid in 2022 seems low vs 2021.
Still, the continued use and mandate of these is why trust no longer exists, and why this round, I’m walking into the Dr’s office to get my kid’s forms signed, but otherwise hands off.

This in my mind is still open for debate, as oldest has dealt with some flavor of ADHD/Autism his whole life, that he is now fortunately is getting a good awareness of and handle on. Vaccine injury? Tylenol injury? Genetic manifestation of something many of my family, including probably myself, has also worked through? Not sure its an answerable question at this point, but grounds for suspicion.
https://www.cdc.gov/meningococcal/images/meningococcal-graph.jpg
https://www.cdc.gov/tetanus/about/index.html#:~:text=Today%2C%20tetanus%20is%20uncommon%20in,all%20the%20recommended%20tetanus%20vaccinations.
https://www.cdc.gov/vaccines/pubs/pinkbook/dip.html#:~:text=Secular%20Trends%20in%20the%20United%20States,-During%20the%201920s&text=From%201996%20through%202018%2C%2014,less%20than%201%20per%20year.
https://www.cdc.gov/pertussis/surv-reporting.html
https://www.lung.org/lung-health-diseases/lung-disease-lookup/pertussis/learn-about-pertussis
https://www.cdc.gov/pertussis/downloads/pertuss-surv-report-2019-508.pdf
https://vaers.hhs.gov
See #2 above, this statement has in mind a plot or two we’ll see in a bit including covid…
https://www.cdc.gov/meningococcal/downloads/NCIRD-EMS-Report-2019.pdf
U.R.F. Yes I know. Similar likely holds for reported cases here too though I’d expect.
Each of my girls had weird fainting, weakness, or blurred visions experiences in middle school. I did get them vaxxed up to that point, but once they started pushing Gardasil when there was little data to support, I stopped taking them to annual appointments. I didn't like how my pediatrician was acting. He couldn't look me straight in the eye. All he could say was if he had a daughter he would have her take it. I have no regrets not getting it for them. None of them had any issues all through high school with no annual appointments or reasons to go to the doctor or urgent care outside of physicals required for sports. I never did flu shots for any of us because I always consider it a moving target.
Thanks Dr Flurm, I am facing this very situation with my 12 year old daughter so very useful information and graphs. I think I will say : hard no